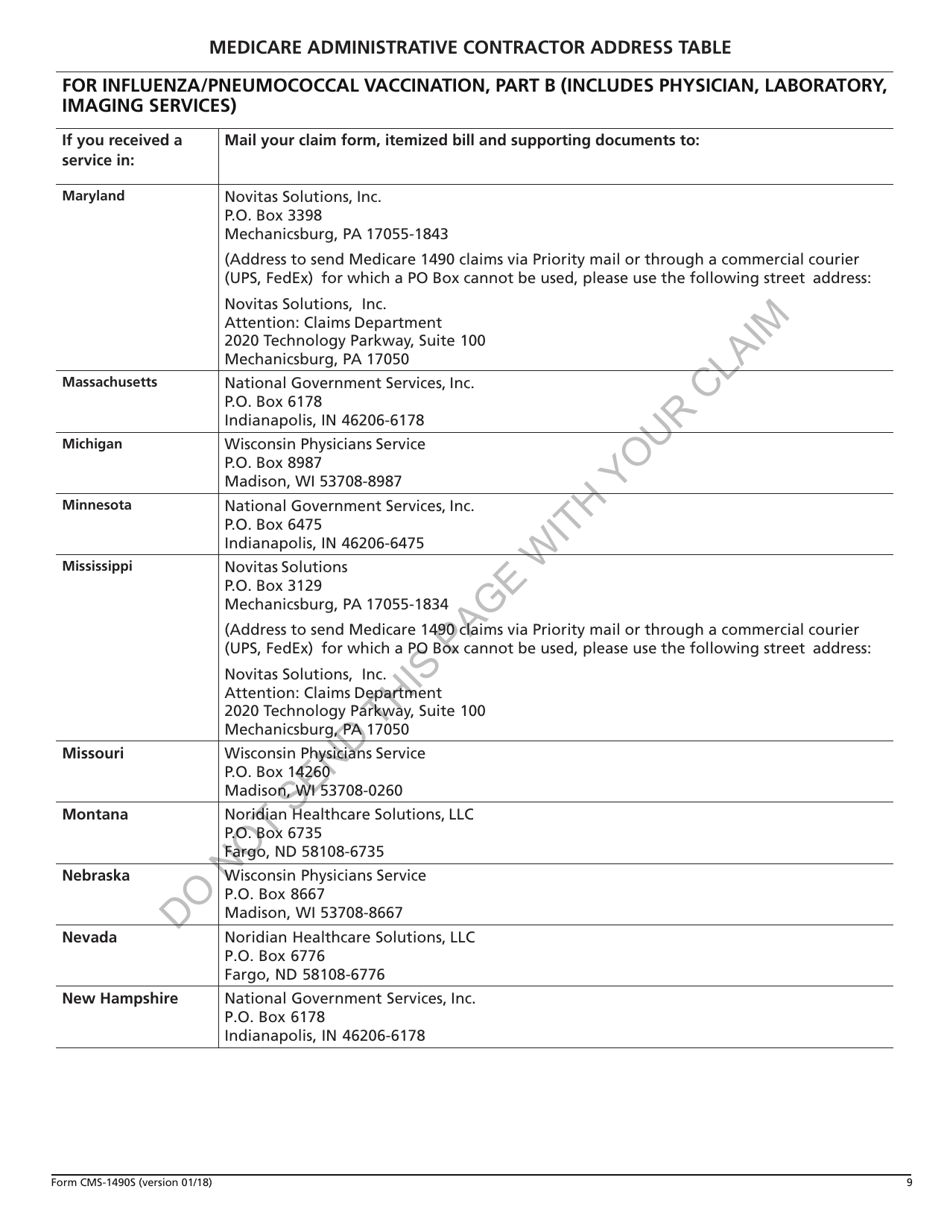
Form Cms 1490S
Form Cms 1490S - If a beneficiary wishes to submit a claim,. Enclosed is the form, instructions for. This form is for sharp health plan medicare members to. Medicare part c member reimbursement request form. Download and print the fillable form cms 1490s to request medicare payment for health care services. Your bill does not have to be. Medicare will pay you directly when you complete this form and attach an itemized bill from your doctor or supplier.
If a beneficiary wishes to submit a claim,. Enclosed is the form, instructions for. Your bill does not have to be. This form is for sharp health plan medicare members to. Download and print the fillable form cms 1490s to request medicare payment for health care services. Medicare part c member reimbursement request form. Medicare will pay you directly when you complete this form and attach an itemized bill from your doctor or supplier.
This form is for sharp health plan medicare members to. Enclosed is the form, instructions for. Download and print the fillable form cms 1490s to request medicare payment for health care services. Medicare will pay you directly when you complete this form and attach an itemized bill from your doctor or supplier. Your bill does not have to be. If a beneficiary wishes to submit a claim,. Medicare part c member reimbursement request form.
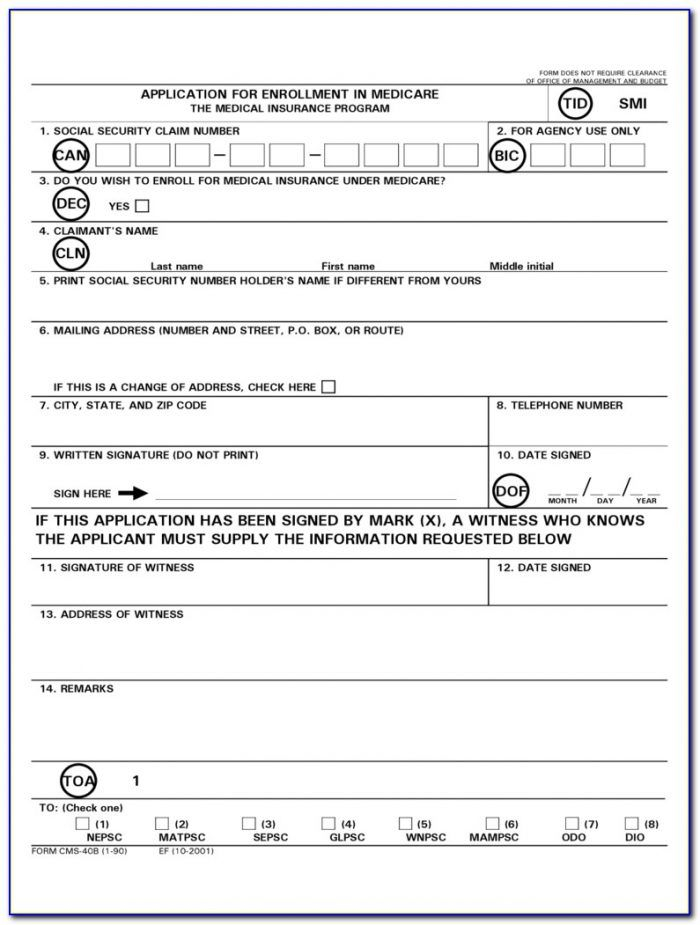
2018 Form CMS40B Fill Online, Printable, Fillable, Blank pdfFiller
Your bill does not have to be. This form is for sharp health plan medicare members to. Medicare part c member reimbursement request form. Medicare will pay you directly when you complete this form and attach an itemized bill from your doctor or supplier. Download and print the fillable form cms 1490s to request medicare payment for health care services.

Medicare Claim Form Cms 1490s Form Resume Examples BX5a6z2OwW
Medicare will pay you directly when you complete this form and attach an itemized bill from your doctor or supplier. If a beneficiary wishes to submit a claim,. Download and print the fillable form cms 1490s to request medicare payment for health care services. Medicare part c member reimbursement request form. Your bill does not have to be.

Fillable Form CMS 1490S Edit, Sign & Download in PDF PDFRun
Medicare will pay you directly when you complete this form and attach an itemized bill from your doctor or supplier. Enclosed is the form, instructions for. This form is for sharp health plan medicare members to. Medicare part c member reimbursement request form. Your bill does not have to be.
Printable Form Cms 1490s Printable Forms Free Online
This form is for sharp health plan medicare members to. If a beneficiary wishes to submit a claim,. Medicare part c member reimbursement request form. Your bill does not have to be. Medicare will pay you directly when you complete this form and attach an itemized bill from your doctor or supplier.
Form CMS1490S Fill Out, Sign Online and Download Fillable PDF
If a beneficiary wishes to submit a claim,. Your bill does not have to be. Medicare part c member reimbursement request form. Download and print the fillable form cms 1490s to request medicare payment for health care services. Medicare will pay you directly when you complete this form and attach an itemized bill from your doctor or supplier.
Medicare Claim Form Cms 1490s Form Resume Examples djVaBnG2Jk
Enclosed is the form, instructions for. Your bill does not have to be. Medicare part c member reimbursement request form. Medicare will pay you directly when you complete this form and attach an itemized bill from your doctor or supplier. If a beneficiary wishes to submit a claim,.
Printable Form Cms 1490s Printable Forms Free Online
This form is for sharp health plan medicare members to. Medicare will pay you directly when you complete this form and attach an itemized bill from your doctor or supplier. Enclosed is the form, instructions for. Medicare part c member reimbursement request form. If a beneficiary wishes to submit a claim,.

Medicare Form Cms 1490s Form Resume Examples BpV5p58Y1Z
If a beneficiary wishes to submit a claim,. Medicare will pay you directly when you complete this form and attach an itemized bill from your doctor or supplier. This form is for sharp health plan medicare members to. Your bill does not have to be. Download and print the fillable form cms 1490s to request medicare payment for health care.
Medicare Form Cms 1490s Form Resume Examples BpV5p58Y1Z
Enclosed is the form, instructions for. If a beneficiary wishes to submit a claim,. Medicare will pay you directly when you complete this form and attach an itemized bill from your doctor or supplier. This form is for sharp health plan medicare members to. Download and print the fillable form cms 1490s to request medicare payment for health care services.

Cms 1490s Fill Out or Print Blank PDF Template Online
Your bill does not have to be. Medicare will pay you directly when you complete this form and attach an itemized bill from your doctor or supplier. Download and print the fillable form cms 1490s to request medicare payment for health care services. Medicare part c member reimbursement request form. This form is for sharp health plan medicare members to.
Medicare Will Pay You Directly When You Complete This Form And Attach An Itemized Bill From Your Doctor Or Supplier.
Your bill does not have to be. Enclosed is the form, instructions for. Download and print the fillable form cms 1490s to request medicare payment for health care services. Medicare part c member reimbursement request form.
This Form Is For Sharp Health Plan Medicare Members To.
If a beneficiary wishes to submit a claim,.